Parasomnias are sleep disorders that involve unusual movements, behaviors, emotions, or autonomic activity during sleep or transitions between sleep and wakefulness. They are common in children and usually harmless, but they can be distressing or disruptive to sleep.
There are two main types of parasomnias:
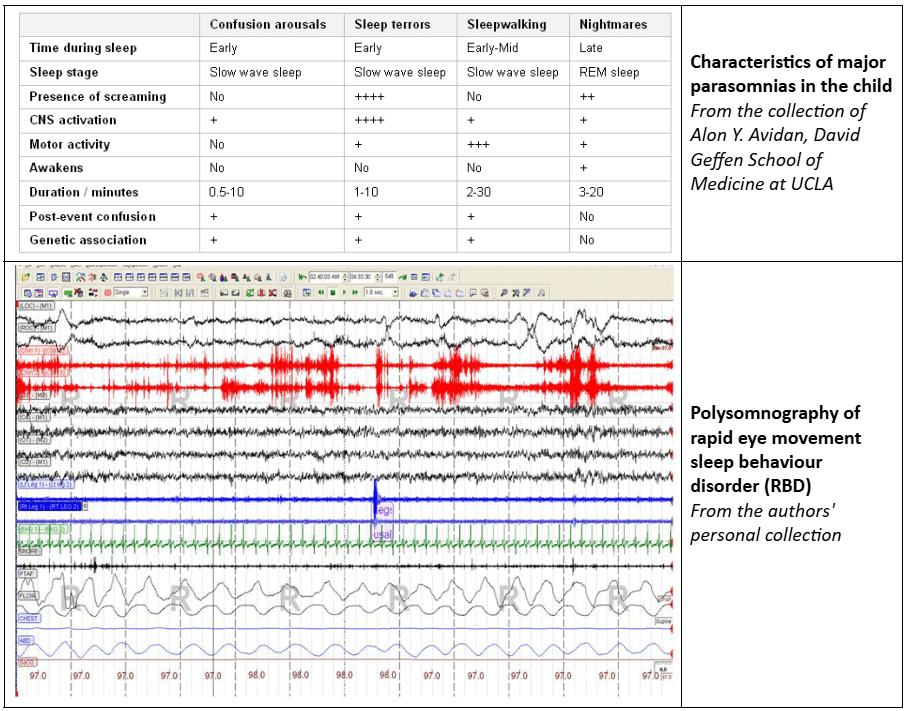
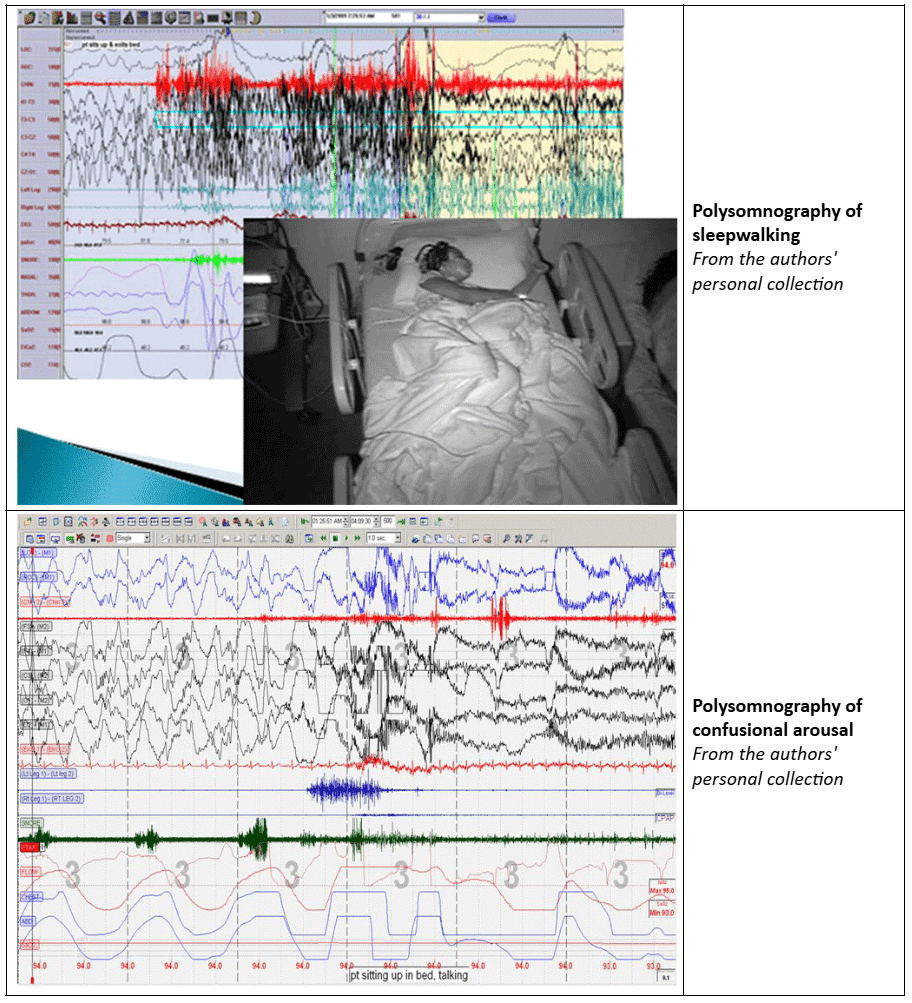
Non-Rapid Eye Movement (NREM) Parasomnias – Occur in the first half of the night and include sleepwalking, night terrors, and confusional arousals.
Rapid Eye Movement (REM) Parasomnias – Occur later in the night and include nightmares, sleep paralysis, and REM sleep behavior disorder (RBD) (which is rare in children).
Most childhood parasomnias resolve on their own, but sleep deprivation, restless legs syndrome, and obstructive sleep apnea can trigger or worsen symptoms. Addressing these underlying causes can help reduce episodes.
Diagnosis and When to Seek Help
Parasomnias are usually diagnosed based on parent or caregiver observations. Parents should consult a doctor if their child:
Has frequent or severe parasomnia episodes that disrupt sleep.
Shows signs of excessive daytime sleepiness, behavioral issues, or difficulty focusing.
Sleepwalks in a way that poses a safety risk.
Has additional symptoms such as snoring or pauses in breathing during sleep, which could indicate an underlying sleep disorder like obstructive sleep apnea.
A sleep study (polysomnography) may be recommended if another sleep disorder is suspected.
Management and Prevention
Most cases of parasomnia do not require medical treatment and improve with good sleep habits and a safe sleep environment.
Ensure Enough Sleep – Maintain a consistent bedtime routine to prevent sleep deprivation, a common trigger.
Create a Safe Sleep Space – Remove sharp or dangerous objects, lock doors and windows, and use safety gates if needed.
Avoid Triggers – Reduce stress, limit caffeine and sugar before bed, and create a calm nighttime routine.
Do Not Wake the Child During an Episode – Gently guide them back to bed if necessary, but avoid trying to wake them forcefully.
In rare cases where parasomnias are severe or persistent, medications may be considered under a doctor’s guidance.
Follow-Up and Monitoring
Keep a sleep diary to track episodes and potential triggers.
Ensure a safe environment to prevent injuries.
Seek medical advice if episodes become more frequent, disruptive, or concerning.
With proper management, most children outgrow parasomnias, and families can take steps to ensure restful, safe sleep.
History and Exam
Key diagnostic factor
Presence of risk factors
Disturbed cognition during event (confusional arousals, sleep terrors, sleepwalking)
Vigorous activity or violent behaviour (confusional arousals, sleepwalking, sleep terrors, and rapid eye movement sleep behaviour disorder [RBD])
Episodes of inability to move (isolated recurrent sleep paralysis)
Other diagnostic factors
Abnormal demeanour and facial expression (confusional arousals, sleepwalking, sleep terrors)
Evidence of injuries
Risk factors
Family history of non-rapid eye movement (NREM) parasomnias (confusional arousals, sleepwalkling, sleep terrors)
Presence of HLA gene DQB1*04 alleles (sleepwalking)
Medication or alcohol
History of psychiatric disorder
Diagnostic Investigations
1st investigations to order
Clinical examination
Polysomnography (rapid eye movement sleep behaviour disorder)
Social and emotional functioning refers to a child’s ability to understand, express, and manage their emotions, as well as to interact effectively with others. These skills are fundamental for building positive relationships, developing empathy, and coping with the everyday challenges of growing up.
Children who experience difficulties in social and emotional functioning may struggle with recognizing their own feelings or those of others, regulating emotional responses, or responding appropriately in social situations. This can lead to challenges such as anxiety, low self-esteem, difficulty making friends, or misunderstandings with peers and adults.
In the school environment, social and emotional difficulties can impact a child’s engagement, cooperation, and overall learning experience. Emotional distress may manifest as withdrawal, irritability, or disruptive behaviour, which can further affect academic progress and peer relationships.
Assessment of social and emotional functioning as part of a neuropsychological evaluation typically includes behavioural observations, standardized rating scales, and information gathered from parents, teachers, and sometimes the child. This comprehensive approach helps identify strengths and areas for support in emotional regulation, social skills, and adaptive behaviours.
Understanding a child’s social-emotional profile allows for the development of tailored strategies to enhance emotional wellbeing, build resilience, and improve social communication. Early intervention and supportive environments can empower children to navigate their emotions more effectively, fostering confidence and meaningful connections.
At Offspring Health, we aim to provide transparent information about the costs involved in neurodevelopmental and educational assessments.
Neuropsychological assessments typically involve multiple sessions that usually take between 8 and 16 hours in total, depending on the complexity and individual needs. Our hourly rate is $260, so the total cost typically ranges between $2,300 and $4,230.
Fees generally cover:
Initial consultation and history gathering
Testing sessions where your child will complete various fun and interactive tasks
Liaison with schools or health professionals as needed
Comprehensive case analysis and report preparation
Feedback sessions with families and, where applicable, educators or other professionals
Please note that standard neuropsychological assessments are generally not covered by Medicare. However, some assessments and therapy services may be funded through the National Disability Insurance Scheme (NDIS) for eligible participants. We recommend discussing funding options with your NDIS planner or support coordinator prior to booking. Private health insurance may offer partial rebates depending on your level of coverage.